

Products and services

Please be aware that this blog contains graphic images of surgery.
There is an unbridgeable experiential and imaginative chasm that separates us from the world of pre-anaesthetic surgery. Whenever I tell people that I work on the history of surgery, much of it in the period before the introduction of ether and chloroform in 1846-7, they often flinch. Even if they do not exhibit a visible affective response, many will express revulsion at the subject matter. ‘I could never do that’ is a common refrain. At the same time, however, there are others who are deeply, perhaps ghoulishly, fascinated by the blood and gore that are associated with surgical pre-modernity.
I would argue that this powerful response, positive or negative, frisson or fright, derives not from a capacity to imagine what it was like to be cut open or sawn apart while conscious, but rather from the very impossibility of conceiving of that degree of pain and suffering. It is not the event that speaks to us, not the experience, so much as the void, the absence of equivalence.
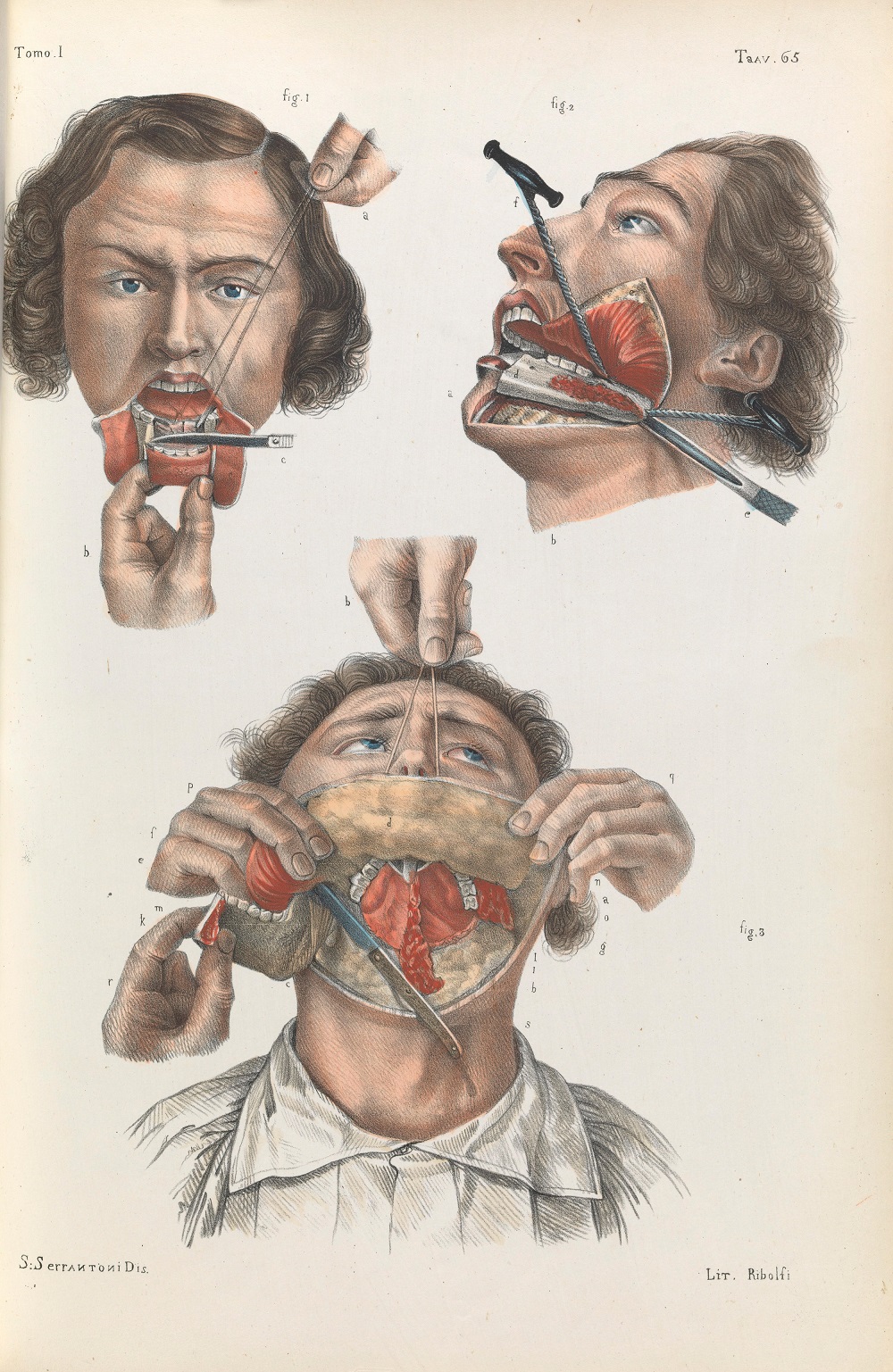
There are good reasons why we cannot connect with the pre-anaesthetic past, why it exists in a realm beyond our comprehension. Most people think of pre-anaesthetic surgery as a crude practice; imagine a patient, jaws clenched in agony, having their leg amputated by an operator in a bloody apron. Certainly, due to the risks of blood loss and shock, surgeons of the period did not, unlike today, intrude too deeply into the body’s main cavities of head, thorax, and abdomen. Yet pre-modern surgical procedures could be far more ambitious and elaborate than we might imagine, as the contemporary image below of the resection of the jaw suggests. How on earth, we might ask, did patients cope with the sensation of having that done to them with no meaningful pain relief?
Beyond the physical qualities of pain, one aspect of pre-anaesthetic surgical experience that has been hitherto neglected is its emotional demands. It is not hard to imagine that the agonies of pre-anaesthetic surgery took a profound emotional toll on patients. Writing to the anaesthetic pioneer James Young Simpson (1811-70) in 1856, the Edinburgh chemist George Wilson (1818-59) recalled the surgical amputation of his foot in 1842, claiming that the emotional trauma of the event had long outlived the memory of physical pain. ‘Of the agony it occasioned I will say nothing’, he wrote:
“Suffering so great as I underwent cannot be expressed in words, and thus fortunately cannot be recalled. The particular pangs are now forgotten; but the black whirlwind of emotion, the horror of great darkness, and the sense of desertion by God and man, bordering close upon despair, which swept through my mind and overwhelmed my heart, I can never forget, however gladly I would do so.” [1]
One did not even have to go ‘under the knife’ to experience powerful emotions. Given the well-recognised curative limitations of pre-modern surgery, especially for conditions such as cancer that were generally detected too late to avert a fatal outcome, patients often expressed feelings of anxiety, dread, and despair, as well as, occasionally, hope, relief, and gratitude.
All these emotions feature in my new book, Emotions and Surgery in Britain, 1793-1912. But in the course of my research I have been especially concerned to address one of the most common misapprehensions in the history of surgery. If the complex emotions of the pre-modern surgical patient are generally recognised (even if understudied), those of the surgeon are not only neglected, but positively denied. It is a widely held belief that pre-anaesthetic surgeons must have been emotionally detached, callous even, in order to cope with the horrors of their art. This image was promoted by surgeons of the later nineteenth century who sought to construct their own modernity in explicit contrast to the ‘dark ages’ of a pre-anaesthetic past. As Frederick Treeves (1853-1923), of ‘Elephant Man’ fame, stated in 1900:
It is little wonder if the older surgeon became rough and stern, if his sense of feeling became dulled, and if the sympathetic side of his nature suffered some suppression. Indeed, contemporary accounts are apt to represent the operator of pre-anaesthetic times as rough almost to brutality and as coarse both in his conduct and in his utterances.[2]
As my research shows, the emotional cultures of pre-anaesthetic surgery were far more rich and complex than such stereotypes suggest. Indeed, contrary to the rhetorical pronouncements of surgical modernists like Treves, emotions played a much greater role in pre-anaesthetic surgery than they do today. The last decades of pre-anaesthetic surgery, from the 1790s to the 1840s, coincided with the era of Romanticism, in which the capacity to experience and reflect on emotional sensation was highly valued, not only artistically, but also culturally, and even scientifically. My book demonstrates the powerful role that Romantic sensibility (that capacity to feel the emotions of others), played in shaping contemporary surgery. Not only did it allow surgeons to shape a culturally resonant identity as gentlemen of feeling, one that elevated them above the traditional image of manual craftsmen, but, by emphasising the emotional authenticity of embodied experience, it enabled them to do so in direct opposition to their traditional professional superiors, the physicians. As the pioneering Edinburgh surgeon John Bell (1763-1820) asked of his rival, the university medical professor James Gregory (1753-1821), in 1800:
“Has his mind been thus keenly touched, almost disordered, at the miseries of his fellow creatures? No, no! his strong sensibilities we hold but lightly: He never passed a sleepless night, reflecting what was to be done on the morrow; never witnessed the severities of the surgeon; never strained hard his breath, nor involuntarily clenched his hands at the sight of another’s agony; nor blanched with fear, nor felt the palpitations of anxiety, in the midst of an eventful operation.” [3]
But emotions were not merely a form of professional posturing; they sat at the very heart of surgical practice and experience. As the example of John’s younger brother, the celebrated anatomist and physiologist, Charles Bell (1774-1842), suggests, the dispositional conventions of Romantic sensibility provided a means to both manage and make sense of the profound sufferings of surgery, not only in the operating theatre but also, in Charles’ case, on the battlefield. They even structured the very perception of the pre-anaesthetic patient as a deeply unstable psychological and physiological entity whose emotional state needed careful management in order to withstand the rigours of operative surgery and ensure an optimal outcome. John Bell is, once again, highly suggestive when he writes that ‘the surgeon must be every thing to his patient; watchful, friendly, compassionate, cheerful; for the patient lives upon his good looks; it is when his surgeon becomes careless, or seems to forsake him, that he falls into despair’.[4] And despair, as any early nineteenth-century surgeon knew, was a prelude to death.
This ‘emotional regime’ of Romantic sensibility was not to last, however. The roots of its demise can be detected as early as the 1820s in the debates around anatomical dissection, and the utilitarian critique of a popular ‘sentimental’ attachment to the corpse. But it truly got underway with the advent of anaesthesia in the mid-1840s. As the patient was now rendered an absent presence in the operating theatre, it was no longer so important to regulate their emotional state. Nor did operations take such an emotional toll on surgeons. As James Miller (1812-1864) put it:
“there can be no doubt that his being compelled to inflict pain, and witness the infliction of it, has always been esteemed by the surgeon as the hardest portion of his professional lot. Now this is gone. He proceeds to operate with a mind wholly unoccupied with regard to the feelings of his patient; for he knows that all the while he will be in unconscious sleep.” [5]
However, it was not until the development of antisepsis from the late 1860s that emotions fully disappeared from surgical practice. In his early lectures, the antiseptic pioneer Joseph Lister (1827-1912) spoke about surgery in the emotive terms of his Romantic forebears. But with his identification of germs as sole the causal agent in the production of post-operative infection, he effectively eliminated the role of emotions in determining surgical outcomes. Patient death was now a chemical rather than a constitutional process.
It was Lister’s associates, acolytes, and hagiographers who crafted the image of pre-anaesthetic surgery that has come down to us. By presenting Lister, and thereby themselves, as the harbingers of surgical modernity, they effectively caricatured the pre-anaesthetic past, robbing it of richness and complexity. This caricature still holds sway and continues to inform surgical self-image. In this way, I hope that my research can not only provide a useful lesson for historians, but also for practising surgeons, who might look at their profession’s past with fresh eyes.
[1] James Young Simpson, Acupressure: A New Method of Arresting Surgical Haemorrhage (Edinburgh: Adam and Charles Black, 1864), p. 568.
[2] Lancet 156:4014 (4 August 1900), p. 314.
[3] John Bell, Answer for the Junior Members of the Royal College of Surgeons of Edinburgh to the Memorial of Dr James Gregory (Edinburgh, 1800), Section II, p. 7.
[4] John Bell, The Principles of Surgery (Edinburgh: T. Cadell Jr and W. Davies, 1801), p. 15.
[5] James Miller, Surgical Experience of Chloroform (Edinburgh: Sutherland and Knox, 1848), p. 29.
Michael Brown is a historian at Lancaster University. He is co-editor of Martial Masculinities: Experiencing and Imagining the Military in the Long Nineteenth Century (2019) and au...
View profile >Keep up with the latest from Cambridge University Press on our social media accounts.







Latest Comments
Have your say!